Leg length discrepancy - Is your pain making you walk around in circles?
The scope of this blog is to shine some light on leg length discrepancy (LLD); a condition that affects the majority of the population. I will outline the types, symptoms, causes, and how osteopathy is effective at managing symptoms.
What is Leg Length Discrepancy?
This diagnosis can either be structural or functional. Structural LLD is when one leg is actually longer than the other due to a difference in bone length. Shortening of one thigh (femur) or calf (tibia) bone can be due to a developmental abnormality in childhood, or it can be a result of trauma, surgery or degenerative diseases (1,2).
Functional LLD is when the legs bones are the same length, but they are positioned so that one leg seems shorter than the other. This could be due to altered lower limb mechanics, spinal scoliosis, or muscle weakness/shortening (1,2). Studies suggest that combined, LLD affects a whopping 90% of the general population, and 40% of athletes (3). The range of discrepancy varies from mild (0-3cm), moderate (3-6cm) to severe (6cm+) (4).
What are the symptoms?
Before I move onto the symptoms; a small side note - A lot of individuals will have a LLD and never know it. If the difference is less than 2cm, the body adapts brilliantly without any need for intervention (3,5). Most people will have a minute discrepancy that will not impact their day to day. The symptoms described below reflect those who are in the moderate to severe categories.
Compensation patterns
So how do we compensate? The body tries its best to adapt to this imbalance, with the shorter leg working to lengthen itself by contracting the calves and quadriceps, straightening the knee and pointing the toes. The longer leg may set in a slight bend. The imbalance becomes really obvious when you take a look at the patient’s hips.
The hip of the longer limb will hitch upwards and backwards, while the other side will sink downwards and forwards; this twist is known as pelvic torsion (3). The body works as a whole unit, so this instability in the lower half of the body will be reflected in the top half of the body to maintain a balance. The pelvic torsion transfers through the lumbar spine, causing the lower back to become irritated and painful, with further twisting up the thoracic spine and shoulders. The shoulder on the same side as the longer leg usually sits lower. These imbalances can result in long term complications such as spinal degeneration and hip arthritis in the longer limb. (6)
Common symptoms of leg length discrepancy:
Lower back pain
Knee pain
Muscle imbalance
Ankle pain
Balance issues
How to Diagnose and Treat LLD
Now, after reading this I’m sure you’ve done the same as me…Stretched your legs out and had a look to see if one foot is sitting further than the other. If the answer is yes, your next question is how do I know if it’s a structural or functional difference?
Well, the gold standard investigation is having a radiographer scan your legs, but assuming you don’t have a CT scanner in your kitchen, simply getting a tape measure and measuring from your hip bone (ASIS) to a prominence on your inner ankle called your medial malleolus, is a reliable way to find your answer (2). If there’s a difference between the legs, it’s a structural discrepancy. If the length is the same but one leg is definitely longer than the other when standing or lying down, it’s functional. Why does this matter? Let’s talk about treatment.

Image courtesy of musculoskeletalkey.com
Treatment of Structural LLD
Mild category individuals fall inside the ‘norm’ of asymmetries and rarely display symptoms of pain or muscle imbalances - Meaning they can be left well alone. Anyone with a significant LLD should be treated on a case by case basis, looking at what symptoms the individuals have. If a 5cm discrepancy causes no pain in the back or hips and the individual is able to undergo their work and hobbies with no issue, then apart from monitoring for changes, no further action is needed. By contrast, if an individual with a 4cm discrepancy presents with lower back pain and knee pain, then treatment is warranted. Symptomatic individuals should start by using shoe lifts (starting small and gradually increasing up to 5cm) for the smaller leg. Shoe lifts greater than 5cm should be avoided, as the degree of instability as a result outweighs the benefit of their use (7).

(8)
Where conservative treatment has failed, one can consider surgical intervention. Surgery involves shortening the longer leg to the height of the short one. This sounds scary, but this option is balanced against the alternative of pain, and long term complications.
Once the leg length is normalised, either by shoe lifts or surgery, it’s important to ‘rebalance’ the body to its new positioning. A body that has developed chronic compensation patterns for a long term discrepancy will not correct overnight - tight muscles remain tight and weak muscles remain weak. Imagine a person with a long right leg, a hitched up right hip, a pelvis tilted forward and downward on the left, a twisted spine and a raised left shoulder, like the man in this cartoon:
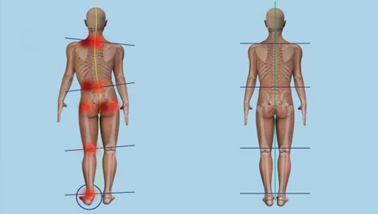
Image courtesy of sportsmedreview.com
This is where the osteopath comes in. We would offer an initial assessment that identifies these compensation patterns. For example, our patient would have a chronically restricted lower spine, a sideways curvature of the mid-spine, a restricted right ankle and right hip, with alternatively tight and weak muscles surrounding these joints. Together, we would come up with a structured management plan that progressively improves range of motion in restricted joints, releases tight muscles in the back, calves and pelvis, and strengthens the adductors, peroneals and glute medius. Careful management of these imbalances provides the body the opportunity to rebalance to a more symmetrical and functional unit.
Treatment of Functional LLD
This treatment is more varied and patient centred, as functional LLD has many different causes that first need to be identified. Common causes include flat feet, weak lateral hip muscles, tight hip flexors and tight spinal stabilising muscles.
The aim is to help restore the pelvis to a neutral position, restoring leg length symmetry. Once releasing the tight tissues, osteopaths look towards the opposing muscles that are subsequently overstretched and weak, providing exercises to strengthen these muscles. Balancing these tight and weak tissues provides stability through the skeletal system, reducing the risk of pain reoccurring.
Final thoughts
To summarise, leg length discrepancy is a complex presentation to manage. Its various causes, symptoms and treatment approaches require case by case examination and a management plan that suits the individual. This aligns with the principles of osteopathy, that demand a patient centred, holistic approach that looks at the patient as an interdependent system, and not as a singular injury.
I hope this blog has helped you understand a little more about leg length discrepancy. If you have any further questions, please feel free to get in touch!
Bibliography
(1) Khamis, S., & Carmeli, E. (2017). Relationship and significance of gait deviations associated with limb length discrepancy: A systematic review. Gait & Posture, 57, 115–123. https://doi.org/10.1016/j.gaitpost.2017.05.028
(2)Khamis, S., & Carmeli, E. (2017). A new concept for measuring leg length discrepancy. Journal of orthopaedics, 14(2), 276–280. https://doi.org/10.1016/j.jor.2017.03.008
(3)Knutson, G. A. (2005). Anatomic and functional leg-length inequality: A review and recommendation for clinical decision-making. Part I, anatomic leg-length inequality: prevalence, magnitude, effects and clinical significance. Chiropractic & Osteopathy, 13(1). https://doi.org/10.1186/1746-1340-13-11
(4) Reid D, Smith B. Leg length discrepancy assessment: accuracy and precision in five clinical methods of evaluation. Physiother Can. 1984;36:177–182. doi: 10.2519/jospt.1984.5.5.230
(5) Applebaum, A., Nessim, A., & Cho, W. (2021). Overview and Spinal Implications of Leg Length Discrepancy: Narrative Review. Clinics in orthopedic surgery, 13(2), 127–134. https://doi.org/10.4055/cios20224
(6) Gordon JE, Davis LE. Leg Length Discrepancy: The Natural History (And What Do We Really Know). J Pediatr Orthop. 2019;39(Issue 6, Supplement 1 Suppl 1):S10-S13. doi:10.1097/BPO.0000000000001396
(7) Campbell TM, Ghaedi BB, Tanjong Ghogomu E, Welch V. Shoe Lifts for Leg Length Discrepancy in Adults With Common Painful Musculoskeletal Conditions: A Systematic Review of the Literature. Arch Phys Med Rehabil. 2018;99(5):981-993.e2. doi:10.1016/j.apmr.2017.10.027
(8) Vogt, Bjoern & Gosheger, Georg & Wirth, Thomas & Horn, Joachim & Rödl, Robert. (2020). Leg Length Discrepancy- Treatment Indications and Strategies. Deutsches Aerzteblatt Online. 117. 10.3238/arztebl.2020.0405.